Researchers Find Noninvasive Brain Stimulation Temporarily Improves Parkinson’s Patients’ Motor Symptoms
Written by |



Noting that while motor movements in people with Parkinson’s disease (PD) generally tend to slow down and decrease in intensity many retain the ability to move more quickly and forcefully, a team of scientists at Johns Hopkins Medical in Baltimore, Maryland, report evidence — gathered from proof-of-concept experiments with joysticks that measure force — that the slowdown likely arises from the brain’s cost/benefit analysis, which gets skewed by loss of dopamine — a chemical released throughout the cortex of the brain by specialized neurons that is known to make animals more likely to exert effort to achieve a reward — in people with PD.
Additionally, the researchers’ study of a small group of 20 patients with PD demonstrated that brain cortex stimulation using external electrodes can correct some of the dopamine deficiency related distortion and temporarily improve some patients motor symptoms.
Parkinson’s disease which affects up to 1 million Americans, is the second most common neurodegenerative disease after Alzheimer’s. A slowly progressing neurodegenerative disorder, Parkinson’s is caused by death of dopaminergic neurons in in a region of the midbrain called substantia nigra for reasons unknown. Dopamine is a neurotransmitter that carries signals between the areas of the brain that regulate and control smooth, purposeful motor movement when performing routine tasks like eating, writing and shaving. Common first symptoms of Parkinson’s include tremors, rigidity and slowness of movement. While the motor symptoms can be treated with medication the disease’s progression cannot be prevented, and benefits of medication may fade as the disease progresses, and/or side effects can become problematic.At the Johns Hopkins Laboratory of Computational Motor Control, headed by Dr. Reza Shadmehr, Ph.D., a professor of biomedical engineering at the Johns Hopkins University School of Medicine, video game-based experiments are a key element in the scientists’ pursuit of understanding how the brain controls movement, allowing performance of complex motions like reaching for a glass of water without even looking, and making them seem effortless.
“Our work focuses on understanding how the human brain perceives the world, how it learns, and how it controls our movements,” explains Dr. Shadmehr. “We study actions of healthy people, as well as people with neurological disorders. We look for regularities and use mathematics to ask about the origins of these regularities. Our approach is non-invasive, aiming to never harm. Our tools include robotics, brain stimulation, and neuroimaging. We have two long-term aims: 1) to understand the basic function of the motor structures of the brain including the cerebellum, the basal ganglia, and the motor cortex; and 2) to understand the relationship between how our brain controls our movements, and how it controls our decisions.”
Dr. Shadmehr is senior author of a report on the research published online in The Society for Neuroscience official Journal of Neuroscience on Sept. 2.
“The loss of dopamine associated with Parkinsons disease makes the effort required to move the affected side of the body seem greater, so the brain is less willing to use that arm to complete tasks,” Dr. Shadmehr continues. “Our study suggests that direct current stimulation can compensate somewhat for the loss of dopamine by decreasing the effort the brain has to put into getting its motor neurons to fire.”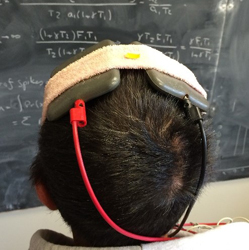
Photo Caption: A volunteer models the noninvasive, electrical stimulation device used in this study.
Image credit – Reza Shadmehr, Johns Hopkins Medicine
The Journal of Neuroscience report, entitled “Altering Effort Costs in Parkinson’s Disease with Noninvasive Cortical Stimulation” (The Journal of Neuroscience, 2 September 2015, 35(35): 12287-12302; doi: 10.1523/JNEUROSCI.1827-15.2015), is coauthored by Dr. Shadmehr and his research colleagues Yousef Salimpour of the Johns Hopkins Department of Biomedical Engineering Laboratory for Computational Motor Control, and Zoltan K. Mari of the Johns Hopkins School of Medicine Department of Neurology.
The researchers observe that in Parkinson’s disease (PD), the human brain is capable of producing motor commands, but appears to require greater than normal subjective effort, particularly for movements on the more-affected side of the body.
In Parkinsons, dopamine neurons generally die on one side of the brain, inhibiting the the patient’s ability of to exert effort with the opposite side of the body. In situations requiring quick reflex action such as preventing a ball from falling off a table, people with PD can often still make rapid, intense movements with their affected arm, but the scientists note that it seems as though the brain’s cost assessment for making everyday movements is abnormally high.
To investigate the nature of this subjective increased effort demand and whether it be altered, they used an isometric task in which patients produced a goal force by engaging both arms, but were free to assign any fraction of that force to each arm. The researchers found that the PD patients preferred their less-affected arm, but only in some directions a preference correlated with lateralization of signal-dependent noise: the direction of force for which the brain was less willing to assign effort to an arm was generally the direction for which that arm exhibited greater noise. They found that consequently the direction-dependent noise in each arm acted as an implicit cost that discouraged use of that arm.
To check for a causal relationship between noise and motor cost, the Dr. Shadmehr’s team used bilateral transcranial direct current stimulation of the motor cortex, placing the cathode on the more-affected side and the anode on the less-affected side. They found that this stimulation not only reduced the noise on the more-affected arm, it also increased the the patients’ willingness to assign force to that arm. In a 3 d double-blind study and in a 10 d repeated stimulation study, bilateral stimulation of the two motor cortices with cathode on the more-affected side reduced noise and increased the willingness of the patients to exert effort. This stimulation also improved the clinical motor symptoms of the disease.
Based on their study’s findings, the coauthors conclude that In Parkinson’s disease, patients are less willing to assign force to their affected arm, and that this pattern is direction dependent: directions for which the arm is noisier coincide with directions for which the brain is less willing to assign force. They hypothesized that by reducing the noise on the affected arm, the brain’s willingness to assign force to that arm may be increased, and one way to do this is via noninvasive cortical stimulation. In addition to reducing effort costs associated with the affected arm, the investigators found that the cortical stimulation also improved clinical motor symptoms of the disease.
To test the hypothesis that dopamine makes animals more likely to exert effort to achieve a reward, Dr. Shadmehr and his team first designed an experiment to measure how much force a patients brain was willing to assign to each arm. In their first experiment, participants, all right-handed, included 15 healthy volunteers and 15 with PD, ages 50 to 75, who had been diagnosed with Parkinson’s for two to 20 years and were receiving medication to control their symptoms, such as tremors, muscle rigidity and lack of balance.
With their arms held in mobile supports above a table, participants were asked to grip handles located at the ends of the supports, which could measure the amount force applied to them. Participants then were asked to apply about four pounds of muscle force to the handles in order to move an electronic cursor on a computer screen to a target. They could use any combination of both arms to achieve the task. This action was repeated 10 times in 16 different directions representing a full circle.
The investigators noted that when performing this task, healthy participants split the four pounds of force between their two arms more or less equally, thereby sharing the effort between both arms, never applying more than 30 percent more force with one arm than with the other. By contrast, patients with PD on average showed a twofold greater preference for their less affected arm, sometimes skewing their effort by as much as 70 percent toward the less affected arm.
Dr. Shadmehr’s team deduced the difference in bilateral allotment of effort was not due to a lack of strength in the PD patients’ affected arms, because the team also tested each arm’s ability to apply force in every direction and found that the patients’ strength comparable to that of healthy individuals.
However what did stand out, the researchers say, was how direction-dependent the outcomes were. For example, when a patient was asked to move the cursor to the 3 o’clock position on the screen, they might entirely favor their left (unaffected) arm. However, when asked to move the cursor to the 12 o’clock position, the patient might share the effort equally between both arms. In addition, the researchers noticed that patients avoided using their affected arm particularly in the directions in which they exhibited a greater amount of variability, or noise, when generating force. That is, the increased effort appeared associated with a poorer ability to control the generation of force.
Hypothesizing that reduced ability to control force in patients with PD was related to decreased dopamine — deficiency of which which makes it more difficult to recruit neurons for a particular task — the researchers devised a brain stimulation experiment to further test their hypothesis.
 “The greater the number of neurons firing together to complete a task, the less they each have to fire and the more controlled the resulting action is,” says Dr. Shadmehr. “In Parkinsons, the loss of dopamine might mean that neurons that control movement dont fire as easily, which means that a few neurons have to do the whole job and cant perform as well, generating noisier output. The brain seems to know this and avoids assigning effort in those directions where it has less control.”
“The greater the number of neurons firing together to complete a task, the less they each have to fire and the more controlled the resulting action is,” says Dr. Shadmehr. “In Parkinsons, the loss of dopamine might mean that neurons that control movement dont fire as easily, which means that a few neurons have to do the whole job and cant perform as well, generating noisier output. The brain seems to know this and avoids assigning effort in those directions where it has less control.”
To overcome this problem, the team used transcranial direct current stimulation (tDCS) — a non-invasive, painless brain stimulation treatment that uses direct electrical currents to stimulate specific parts of the brain — on a total of 25 patients, 10 for each of three tests, with some participating in more than one test. The investigators reasoned that by increasing the electrical current within the neurons using mild stimulation through electrodes placed on the scalp, the cells would be closer to their firing threshold and would be easier for the brain to engage.
As explained in a Johns Hopkins release, in tDCS a constant, low intensity current is passed through two electrodes placed over the head which modulates neuronal activity. There are two types of stimulation with tDCS: anodal and cathodal stimulation. Anodal stimulation acts to excite neuronal activity while cathodal stimulation inhibits or reduces neuronal activity. And although tDCS is still an experimental form of brain stimulation, the scientists say it potentially has several advantages over other brain stimulation techniques — being as it is cheap, non-invasive, painless, safe, and easy to administer with easily portable equipment. They note that most common side effect associated with tDCS is a slight itching or tingling on the scalp, and that several studies suggest that tDCS may be a valuable tool for the treatment of neuropsychiatric conditions such as depression, anxiety, Parkinson’s disease, and chronic pain. Research has also demonstrated cognitive improvement in some patients undergoing tDCS, but currently, tDCS is not an FDA-approved treatment.
In another, blinded experiment involving 10 patients, in which neither patients nor evaluating clinicians knew which kind of stimulation they received, the investigators found that cathodal tDCS, worked best and that the patients who received cathodal stimulation were more willing to engage their affected arm than those who received no stimulation, or anodal stimulation. The researchers also observed a related decrease in the variability associated with these patients’ movements, noting that the stimulation produced an average improvement of 25 percent in patients’ motor symptoms as quantified via the motor component of the Unified Parkinsons Disease Rating Scale (UPDRS), particularly improving rigidity on the affected side.
Finally, the researchers tested tDCS effectiveness in 10 patients over a 10-day period. During the first three days, participants received no stimulation or fake stimulation; on days four through eight, they received cathodal stimulation; and on days nine and 10, no stimulation. Each day, they executed the arm movement test and the UPDRS. Results of the experiment showed that improvement was real but temporary, only occurring on the days the patients received cathodal tDCS.
“As far as we know so far,” Dr. Shadmehr cautions in a Johns Hopkins Release, “the effects of tDCS are very temporary, but that’s not surprising since no new dopamine cells are being created, which is the root of the problem. Nevertheless,” he says, “tDCS is a relatively simple, painless and inexpensive intervention that could be developed for home use, a device we are working on.”
“Its possible,” he adds, “that the brain would get used to the stimulation just as it adjusts to medications and also become less responsive over time, but we are hopeful that continued stimulation might improve symptoms.”
This work was supported by grants from that National Institute of Neurological Disorders and Stroke (NS078311) and the Human Frontiers Science Program.
Sources:
Johns Hopkins University School of Medicine
The Journal of Neuroscience
Image Credits:
Reza Shadmehr, Johns Hopkins Medicine
Sources:
Johns Hopkins University School of Medicine